
January 2005, Vol. 15, No. 1
Body Weighting for Postural/Structural Correction
INTRODUCTION
The use of head and body weighting, for the purpose of postural and structural correction, is becoming increasingly popular with Chiropractors. Unfortunately, good objective information regarding its history and use are hard to find. Because of this, I have taken the time to research and present a brief history of body weighting and some of my own observations regarding its clinical use.
BRIEF HISTORY
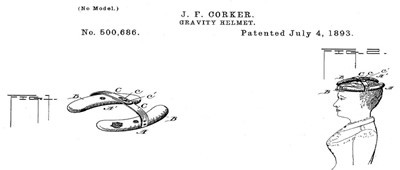
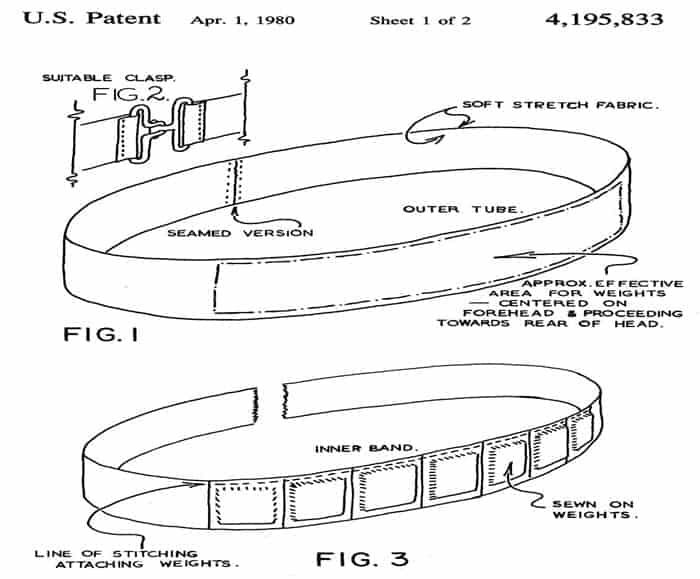
The oldest patented head weighting device that I could find dates back to July 4, 1893 (See picture A). It was called a Gravity Helmet and was invented by J.F. Corker.1 Since then, numerous types of head or body weighting have been patented. (See pictures B, C)2,3 All of these innovative designs were intended to strengthen and balance the muscles of the neck/body and improve overall head and body saggital posture. The first forehead worn head weight, like what is commonly used today, was designed by Jean Svendsen and was patented on April 1, 1980. (See picture D)4 The first appearance of body weighting in the medical literature was in “Scoliosis, Diagnosis and Management” by Doctor Rene Cailliet.(See picture E)5 This text was published in 1975. The first use of body weighting in a published research paper occurred in 2003 and was authored by researchers associated with the Pettibon Biomechanics Group.6 Doctor Burl Pettibon has advocated head and body weighting since the early 1990’s.7 Unfortunately, his recently patented method of body weighting8 leaves some important questions unanswered. Questions such as:
- Which saggital neck configurations are good for head weighting and which are not?
- Who is body weighting most effective on and least effective on?
There are other aspects of Dr. Pettibon’s patented methods that I, respectfully, do not agree with. In the hope of bringing some objective light to this subject, I would like to provide you with by own observations after five years of clinically utilizing ambulatory body weighting for the purpose of postural and structural correction.
CLINICAL OBSERVATIONS
- Body weighting appears to trigger the body’s natural righting reflexes to induce a directly opposing, Mirror-Image®, translation of the weighted structure. This translation is in relation to the body portion directly below it (i.e., head to thorax, thorax to pelvis, pelvis to feet). A small weight produces a small translation motion; a larger weight produces a larger translation motion to occur. Sometimes more than one body portion can be affected by the body weight.
- It is possible to over head weight the patient and cause their head posture to fail by dropping forward and into flexion, rather than retracting to a more normal posture. Over body weighting the torso can also cause posture failure to occur.
- Body weighting always induces some degree of directly opposing, Mirror-Image® translation to occur. Because of this, always weight the side of translation. If two translations are involved, combine them for optimum correction (i.e. right head translation with forward head posture = place head weight over the right eye).
- Body weighting appears to be most effective in the young and flexible. Children and adolescents can make amazing A-P and/or lateral translation corrections with as little as one month of three times per week, in-office 15 minute ambulatory treatments on a treadmill. The older, more structurally degenerated and/or more fibrotic the individual, the less effective body weighting appeared to be and the more effective Mirror-Image® traction and active Mirror-Image® exercise and adjustments appeared to be. In fact, if I place a body weight on an older patient and do not see a notable postural change occurring, I do not have them perform the therapy.
- Patients past their teens who structurally qualify for body weighting therapy require more than three-times-per-week of in-office 15-minute ambulatory treatments to really affect correction if body weighting is the primary form of rehabilitative therapy. I encourage my older patients to try and work-up to at least two 15-20 minute ambulatory sessions per day.
- Head weighting applied in small amounts (2-3 lbs.) appears to trigger a subtle contracture of the sub-occipital muscles to such a degree as to produce a retraction of the upper cervical segments back towards the CBP® ideal arc line when the lower segments are in a relatively normal position (See Picture F).
- Head weighting applied in larger amounts (4-6 lbs.) appears to trigger a full head and neck retraction with the expected upper cervical flexion and lower cervical extension. This is fine for patients with large forward head posture that present with the normal postural coupling patterns of upper cervical over-extension and lower cervical flexion.
- Head weighting should not be applied to individuals who present with their lower cervical segments in marked extension of the CBP® ideal arc line. Anterior head weighting of these people will only aggravate the already over-extended lower cervical facet joints and not improve their saggital cervical structure.
- Young or middle-aged patients who do not present with buckled, kyphotic, extended cervical or lumbar spines, are often good candidates for corrective body weighting. I believe the average young patient’s postural/structural problem is often more neuro-muscular and not so much musculo-ligamentous. Especially if there is no history of repeated or pronounced trauma. If in doubt, take a new x-ray with the patient wearing the body weight that produces the best visual postural correction and see if it induced a structural improvement or Mirror-Image® reversal. If it has, then I believe that continued use of the body weight could correct the structural problem better than musculo-ligamentous traction. If only a partial correction is achieved on the body weighted x-ray, then obviously both therapies (traction and body weighting) are required.
- A neuro-muscular postural problem left un-corrected for a long enough period of time will progressively become a musculo-ligmentous postural problem.
CONCLUSION
I personally believe that body weighting has a tremendous potential to assist in the correction of structural and postural problems, especially in the young and middle-age, flexible patients who are sometimes disappointed with the results traction alone can produce. It is my sincere desire that the presentation of my clinical observations will assist practitioners and encourage further research into the short and long term effectiveness of body weighting therapy for structural and postural correction in the appropriate patient population. I hope to present a more detailed history and a few clinical case studies at the upcoming 2005 CBP® Annual in Chicago.
REFERENCES
- Corker J. Gravity Helmet. U.S. Patent #500,686, July 4 1893.
- Hamilton A. Physical Developer. U.S. Patent #1,047,212, Dec. 17, 1912.
- Forrest Sr. C, Stump J. Fluid-Filled Neck Exerciser. U.S. Patent #4, 988,093, Jan. 29, 1991.
- Svendsen J. Facial Exercise Aid for the Face, Neck and Jaw. U.S. Patent #4,195,833, April 1, 1980.
- Cailliet R. Scoliosis, Diagnosis and Management. F.A. Davis Company, Philadelphia, PA, 1975.
- Saunders S, Woggon, D, Cohen C, Robinson D. Improvement of Cervical Lordosis and Reduction of Forward Head Posture with Anterior Head Weighting and Proprioceptive Balancing Protocols. J Vert Sub Resh, April 27, 2003, p 1-5.
- Woggon D. References Must Support Article. Letters to the Editor, Posture Magazine, PBI Inc., Vol. 1, #4, Nov/Dec 2003, p. 3.
- Pettibon B. System for Spinal and Posture Examination and Treatment. U.S. Patent #6,788,968, Nov. 14, 2002.
Picture A
Picture B

Picture C

Picture D
Picture E






